Eyesite cornea surgeon Simon Levy specialises in treating keratoconus. This article explains the condition and how he provides the most modern therapies such as laser, collagen crosslinking, Intacs and partial cornea transplantation.
What is keratoconus?
Keratoconus is a disorder of the cornea the transparent front window of the eye. The cornea focuses light so any abnormality of its shape will reduce vision. Normally it has a smoothly curved surface like a tennis ball. In keratoconus the cornea is distorted by a protrusion shaped like a microscopic volcano: as it is only fractions of a mm high it cannot be felt or seen, except in severe cases.

Normal cornea profile (left) is smoothly curved. Keratoconic cornea (right) is distorted

Structure of normal eye

Normal cornea profile (left) is smoothly curved. Keratoconic cornea (right) blurs image
Symptoms of keratoconus
The main symptom is blurred vision
Keratoconus usually begins in the late teens to early 30s and affects men and women. It is significant for 1:2000 people but mild cases occur up to ten times more often. One or both eyes may be affected. It may begin in one eye and later involve the other.
The main symptom is blurred vision even in glasses. The glasses prescription increases with time and usually shows high levels of myopia (short sight) and astigmatism. Some patients have glare driving at night or from sunshine.
If the distortion of the cornea worsens, so will vision. This happens in some patients but in many the condition stabilises. It is not possible to predict whether keratoconus will be progressive or at what rate it will worsen but in general the younger the age and the more severe the disorder when it begins, the more rapidly it is likely to deteriorate.
In advanced cases hydrops can occur: this is the sudden onset of discomfort, redness and reduced vision caused by a split in the inside of the cornea. It usually clears after a few weeks but may leave permanent scarring. A proud nebula is a small white scar at the tip of the keratoconic protrusion: it may worsen vision and glare and decrease contact lens comfort.
Cause of keratoconus
In most cases of keratoconus the cause is unknown
Keratoconus sometimes run in families. Persistent heavy eye rubbing may be a risk factor but it is not otherwise lifestyle-related. It is slightly more frequent in severe asthma or eczema and patients with chromosomal disorders such as Down's syndrome quite often have keratoconus.
Diagnosis of keratoconus
Diagnostic equipment includes a cornea topographer
The protrusion on the cornea may be seen with a slit lamp microscope. Retinoscopes and keratometers are used to measure eyes for glasses and contact lenses: in keratoconus they show abnormal readings. The cornea topographer is the most important diagnostic device: it makes a map of the cornea surface and accurately measures the keratoconic protrusion.

The Galilei topographer

Topography of normal cornea (left) shows mostly green and yellow colour in the centre. Contrast with a keratoconic cornea (right) where the volcano-like protrusion shows as a red colour
Treatments for keratoconus
New technologies have improved the treatment of keratoconus
Until recently, patients have worn contact lenses unless they needed a cornea transplant – there was no choice and no way of stopping keratoconus from getting worse. Fortunately several important new treatments are now available. Here is my approach
Contact Lenses
The standard treatment
Contact lenses do not change the keratoconus, but cover the protrusion on the cornea so neutralising it. Gas permeable (rigid) contact lenses are usually needed but sometimes special types of soft lenses work. Normal vision is restored to all except advanced cases. Lifelong wear is necessary. Unfortunately it may be difficult to fit a contact lens over the protrusion and wearing it may be uncomfortable.
Collagen crosslinking
A transformation in keratoconus treatment that stops it from getting worse
What is it? – Collagen crosslinking is an important new treatment that stops keratoconus from getting worse. As it does not reduce keratoconus that is already present, it follows that it is best done at an early stage. Most patients need only one treatment per eye, but it may be repeated if necessary. It is done under local anaesthetic (eye drops) in outpatients and does not require hospital admission.
How may benefit be maximised? – After collagen crosslinking has been done to stabilise keratoconus, vision may be improved by laser, Intacs implants and phakic intraocular lenses.
How long has it been available? – The technique was developed in 1998 in Germany.
How does it work? – The cornea is composed of collagen. In keratoconus the collagen is weak, for unknown reasons. Crosslinking increases the strength of the collagen in keratoconic corneas by 3–4 times. Collagen fibres, previously separate, are bonded together crosslinked) by a chemical reaction. This is done by applying vitamin B2 (Riboflavin) as an eye drop and then exposing the cornea to ultra- violet light from a medical device intended for this function.
Before crosslinking

After crosslinking

Cornea Collagen – there are more bonds (shown as red disgonals) between the collagen molecules of the cornea after than before treatment, so strengthening the cornea and stabilizing its shape
What are the risks? – Collagen crosslinking has an excellent safety record. Three regions of the eye that might be damaged are 1. the endothelium, which is protected from the UV light so long as the cornea is about 450 microns thick. Although many keratoconic corneas are thinner than this, there is a simple technique to temporarily swell the cornea just before treatment so the procedure may still work with thinner values. 2.& 3. The lens and retina. These are not affected by the ultraviolet light because the Vitamin B2/Riboflavin eye drops applied to the cornea absorb it, preventing onward transmission and because crosslinking devices are designed to focus the UV light on the cornea only.

Riboflavin (vitamin B2) – chemical composition

The Vega cross linker
Laser
A high-tech new treatment to improve vision
Laser may now be used to treat some cases of keratoconus. The technique is similar to the Lasek laser done for short sight etc, but uses a cornea topographer to guide the laser. In medical jargon this is 'topography-driven treatment'. The laser reduces the keratoconic protrusion, improving vision. When controlled by a topographer only a few microns of cornea need be removed, greatly enhancing safety. The technique is effective for mild-to-moderate keratoconus. To stabilise the cornea after laser, collagen crosslinking is done.

The excimer laser is used with a 'topography-guided' module for keratoconus
Intacs implants
An established treatment for more advanced keratoconus
Intacs are two small pieces of plastic inserted into a channel created in the cornea. They can't be felt and require no maintenance. They are normally invisible except on close inspection when they look like a contact lens on the eye.
The implants work by evening out the keratoconic protrusion, so improving vision. The technique works best for moderate-plus keratoconus. Improvement varies between patients and may be enhanced by laser and phakic intraocular lenses.
In 2000 I was one of the first surgeons in the UK to use Intacs, initially for patients who were short sighted but whose eyes were otherwise normal. I have treated keratoconus with them since 2002 and was an expert adviser to the National Institute for Clinical Excellence (NICE), which has endorsed their use. They are also approved by the Food and Drug Authority (FDA) in the USA.
An advantage of Intacs are that they are reversible as the implants can be removed (by the doctor) and the cornea returns to its previous state. No cornea is removed during insertion ie: the technique is rather than subtractive. Reversibility may be helpful when new technologies for treating keratoconus become available.

Two Intacs implants rest on a fingertip (left). Intacs (right) after insertion (simulation)

Intacs implants in the cornea
Phakic intraocular lens
An effective treatment after cornea shape has been normalised
This is a minature focusing lens, inserted via a keyhole incision. It is held permanently in place on the iris (coloured part) of the eye by special attachments. It works together with the eye’s natural lens which is not removed. In a normal cornea it is capable of correcting even the most severe short sight and astigmatism. In keratoconus it is most effective after collagen cross linking, laser or Intacs have been done to stabilise the cornea and normalise its shape as much as possible.

A phakic intraocular lens (left) is implanted eye and attached to the iris (right). It is invisible under normal circumstances
Proud Nebulae
Removal improves vision and comfort
These can usually be removed by a simple procedure, improving vision and contact lens comfort and reducing glare.
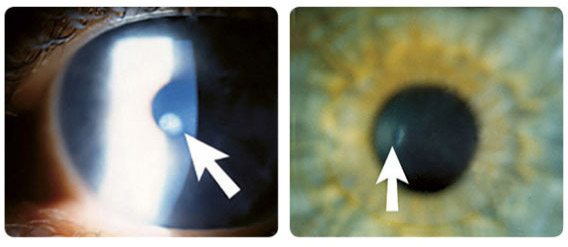
A proud nebula (left) is seen as a white scar on this keratoconic cornea. Keratoconic cornea (right) after removal of proud nebula. Only a faint impression of the scar remains (arrow)
Partial cornea transplantation
Sophisticated transplantation with a low risk of rejection, for advanced keratoconus
This new method saves some of the patient's own cornea and only replaces the outer layer. This is ideal in keratoconus because usually only the outer layer of the cornea (the stroma) is abnormal whilst the inner layer (the endothelium) is healthy. Preserving the patient's healthy endothelium is important as it greatly reduces the risk of transplant rejection.
The technical name for this procedure is deep anterior lamellar keratoplasty.
I always perform partial transplantation when possible. However if the keratoconus is too advanced, for example the cornea is severely scarred, full thickness transplantation is done instead.
Gas permeable contact lens wear may be necessary after the surgery.
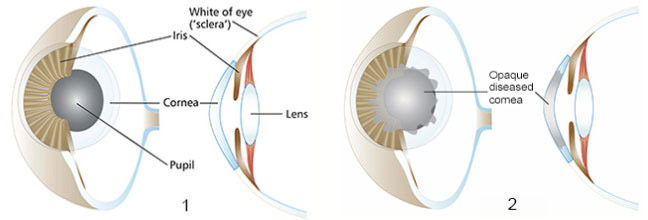
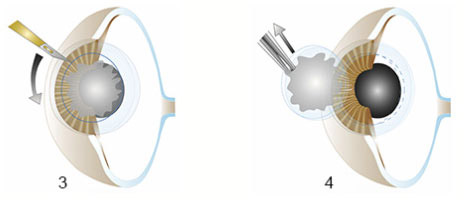
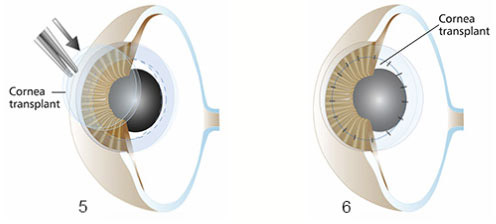
These illustrations of partial cornea transplantation (deep anterior lamellar keratoplasty) are a general guide, not an exact description.

1. In health, the cornea is perfectly clear.
2. The technique is suitable when keratoconus only involves the outer layer of the cornea
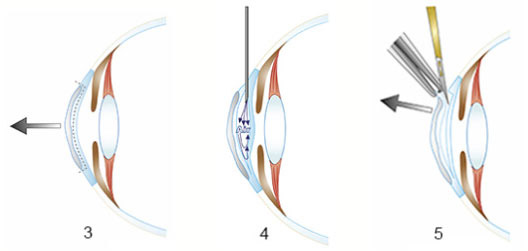
3. The diseased outer layer of the cornea will be removed and replaced.
4. Air is injected into the cornea to seoarate the two layers.
5. The abnormal layer is completely removed
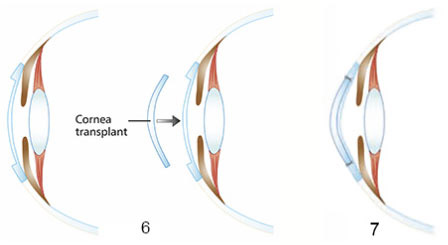
6. A healthy cornea is transplanted into the patient's cornea to replace the diseased layer.
7. The cornea transplant is secured with ultra-fine sutures
Full thickness cornea transplantation
A long-established treatment for the most severe cases
The centre of the patient's own cornea is completely removed and replaced by a transplant. This is the longest-established treatment for severe keratoconus. It is appropriate when all the cornea is abnormal, not only the outer layer.
The technical name for this procedure is penetrating keratoplasty.
Risks include rejection of the foreign tissue by the patient's immune system (greater than after partial transplantation but still infrequent), wearing out of the transplant after many years and astigmatism (an uneven corneal shape) post-operatively requiring gas permeable contact lens wear.
These illustrations of full thickness cornea transplantation (penetrating keratoplasty) are a general guide, not an exact description.
1. In health, the cornea is perfectly clear.
2. The technique is suitable when keratocunus involves the full thickness of the cornea
3. A circular cut is made into the diseased cornea.
4. The diseased cornea is removed
5. A healthy cornea is transplanted into the space created by removal of the patient's diseased cornea.
6. The cornea transplant is held place with ultra-fine sutures. These are not visible to the naked eye. The transplant bonds slowly to the patient's cornea and the sutures are then removed

I performed this full thickness cornea transplant for a patient with advanced keratoconus
